


Adventures in market shaping
Why the pneumo AMC isn't the primary source of learning from global health for the future of the CDR industry

Last week I kicked off a series of posts centered around the opportunity that Frontier has to shape the emerging market for carbon dioxide removal, as we set off on the quest to build a gigaton-scale CDR industry from scratch before 2050. My first piece compared and contrasted the Frontier AMC with the pneumococcal vaccine AMC that helped inspire it.
My next and last two posts in the series will get to the punchline question: how might Frontier use its tremendous leverage to shape the CDR market most powerfully and creatively over the coming decade?
But before getting to that punchline question, today’s post zooms out to consider what else in the recent history of global health might be relevant to the future of the burgeoning CDR market. Over the past two decades, “market shaping” has emerged as a discipline we now routinely use to catalyze big new markets for healthcare products in the developing world and simultaneously steer these markets toward healthy dynamics. Though Frontier has highlighted the pneumo AMC example to the climate tech community, the pneumo AMC has a generally-positive-yet-mixed reputation in the global health world and has been just one of many tools in the market-shaping toolkit that the global health community has developed. Indeed the CDR market has a lot more to learn from the wider recent history of global health market shaping than it does from the pneumo AMC itself.
The history of HIV/AIDS treatment in low-income countries is a particularly illuminating case study. Just as we hear lots of skepticism today about gigaton-scale CDR, as recently as twenty years ago the notion of getting life-saving treatment to tens of millions of HIV+ people in the Global South met with widespread cynicism. Many thought leaders felt we should be focusing our efforts on preventing HIV transmission and that attempting to expand treatment access would be a misguided distraction. Constraints to scaling up treatment abounded: inadequate funding, healthcare worker shortages, unreliable supply chains, and more. Often the first thing people would seize on and frame as an insurmountable barrier was high drug prices. Just like DAC today might cost $500-1,000/ton, prices for life-saving antiretroviral (ARV) drugs in the infant-stage generic ARV drug market exceeded $1,000 per patient per year.
Fast forwarding to today, nearly 30 million people—roughly three-quarters of HIV+ people around the globe—are now on treatment. Drug prices have plunged to <$75 per patient annually, new funding has flooded in, supply chains have dramatically improved, and other roadblocks have been tackled. Like the eradication of smallpox, the dramatic scale-up of global HIV treatment has been an amazing and still under-appreciated human success story. How did this happen?

In what follows, we’ll take a deeper look at what happened in the ARV market in particular. The HIV treatment scale-up miracle is a much wider story with a huge cast of characters; but building and shaping a big ARV market with healthy dynamics was a sine qua non in expanding treatment access and the most relevant to CDR.
We’ll first walk through three successive phases of the ARV market’s evolution, looking at what it took to get from market infancy to a mature, thriving market. I mostly, though not exclusively, discuss the role that the Clinton Health Access Initiative (CHAI) played. CHAI coordinated much of the early ARV market-shaping effort and pioneered most of the tools and tactics that are commonly used today. It’s also a story I know from the inside, having served on CHAI’s executive team during the early days of HIV treatment scale-up before it became the 1700-employee organization it is now.
From there, I zoom out and unpack six major thematic learnings that are applicable as we try to follow a similar path with carbon removal. If you have limited time, skim the next section and then read the final section. I couldn’t figure out how to convey the key parallels effectively without a bit of a history deep dive, so bear with me.
The Evolution of the Developing World ARV Drug Market
Phase 1: Overcoming the chicken-and-egg problem
HIV treatment saves—and changes—lives. Before-and-after photos, like these of Dr. Paul Farmer’s friend and patient Joseph Jeune, tell the story:
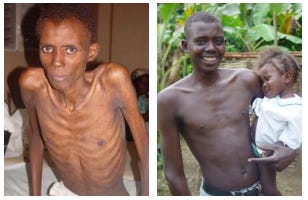
To get people to begin imagining in 2002 that a massive roll-out of treatment was going to be possible, we first had to help the global community imagine that it could become affordable. Yet the ARV drug market was trapped in a chicken-and-egg dynamic. Generic suppliers couldn’t manufacture the drugs at large volumes—and thereby climb the learning curve while gaining economies of scale to achieve progressively lower costs—if demand from developing countries remained low. Meanwhile those same countries couldn’t imagine building big public HIV treatment programs if the drugs stayed insanely expensive.
An AMC would have helped break this chicken-and-egg stalemate, but the concept wouldn’t be pioneered until the pneumo AMC came around years later. Instead, CHAI stepped in to help solve the dynamic in a different way.
Essentially, CHAI engaged the first wave of potential customers and potential suppliers to get everyone engaged in a collective imagination experiment. CHAI asked customers to imagine what they might do in a hypothetical world where ARV prices started to fall quickly: would you start building the beginnings of a meaningful-scale national HIV treatment program? Likewise, CHAI asked suppliers to imagine what they might do if substantial customer orders started flowing in: would you take the risk of investing in new manufacturing capacity and offering prices premised on manufacturing at larger scale?
Sequentially, the first step was to help the early customers—a group of thirteen governments in Africa and the Caribbean—form a buyers club and build models to forecast how they could afford to scale up national HIV treatment programs if drug prices started to fall. CHAI then rolled up those plans into an aggregate forecast of the buyers club demand and took the resulting summary to a group of four generic drug manufacturers in India. These suppliers were notionally interested in producing ARVs, but were skeptical that a market would materialize. Equipped with a much more credible picture of early demand evolution, CHAI negotiated with suppliers and asked them to take the first leap of faith—asking them to project cost levels at the implied production volumes 12-18 months down the road, and offer corresponding prices to the buyers club today as a way to get the market kickstarted.
The outcome was a landmark deal announced in October 2003, committing the participating suppliers to ARV price ceilings as low as $140 per patient per year for the cheapest available regimen.
Phase 2: The early years of scale-up
The deal helped get things moving. Over the next few years, a virtuous cycle kicked in, where the lower prices boosted demand and thereby production volumes which pushed down costs and prices further, and so on it went.
Other tailwinds were picking up. Groups like Partners in Health (PIH) and Médecins Sans Frontières (MSF) demonstrated how transformative clinical outcomes were possible even in the hardest places, and activists pounded the pavement. Jim Kim, who co-founded PIH with Dr. Paul Farmer, joined the WHO to lead its HIV/AIDS response and sought to rally the worldwide community around a “3 by 5” goal: an aspiration to get three million people on HIV treatment by 2005. At first many laughed this off as impossibly optimistic, but the boldness of the rallying cry helped spur everyone to aim higher. The Global Fund launched in 2002 and the U.S. later announced its PEPFAR plan to invest $15 billion in US aid to developing-world HIV programs over five years. The goalposts were starting to shift, and ambitions gradually became more commensurate with the urgency and scale of the problem.
Yet two things were true of this multi-year phase. At one level—similar to the “green vortex” dynamic Robinson Meyer has written about—the market started to make itself, to snowball through the virtuous price/demand cycle toward something bigger. At another level, a range of troublesome dynamics started to emerge in the market including:
Lingering perceptions that generic ARVs were not of truly equivalent quality to ARVs produced by the originator companies (Merck, Bristol Myers Squibb, etc.)
Slow market penetration of next-generation ARVs offering better efficacy, convenience and or side-effect profiles
Predatory pricing behaviors among some suppliers
Cautious tendencies on all sides of the market that left clear untapped potential to speed up the growth of the market and push down the cost curve
Within CHAI it became clear that getting over the initial chicken-and-egg problem hadn’t been enough. CHAI and its partners needed to build a new and wide-ranging capability to shape the ARV market aggressively toward the thriving, healthy, huge market we knew it could become.
On the supply side, CHAI helped manufacturers accelerate their march down the cost curve. Its efforts focused on next-generation ARVs that had become the gold standard in wealthy-country HIV treatment but were just starting to enter the picture in the developing world. CHAI used its leverage (and the trust gained by unlocking a new market opportunity) to get suppliers to open their books and forensically explore ways to squeeze out cost. If, for example, 10% of the cost structure for a particular drug’s active ingredient came from one particular speciality chemical sourced from China, CHAI would have a team on a flight the next week to go meet with that upstream supplier and negotiate a bulk discount for our partner ARV suppliers. Led by the famously tough-love negotiator Ira Magaziner, CHAI got suppliers to agree to regularly updated ‘cost-plus’ pricing, setting prices based on anticipated costs plus a modest but sustainable margin.
What I remember from this time is that the bigger the barriers we encountered, the more we pulled out all the stops we could dream up. For the hardest niche categories within the ARV market—notably pediatric ARVs and so-called “second line” drugs—CHAI partnered with a new innovative finance mechanism called UNITAID to run catalytic pooled-procurement programs (essentially eight- or low-nine-figure mini AMCs). These programs, funded by UNITAID and implemented by CHAI, induced suppliers to pursue new products in these market niches and get over the initial low-volume/high-price hump. In parallel, CHAI built out a team of world-class process chemists to help suppliers improve their yields at the crux stages of active ingredient manufacturing processes. We had never set out to become experts on things like novel asymmetric additions of acetylides to trifluoromethyl ketones, but that was where the journey took us.
Though CHAI initially built its name around supply-side work, the true power of its market shaping lay in its growing ability to carry out shuttle diplomacy and relentless barrier-whacking across all sides of the market. Over a period of years, CHAI established an even bigger demand-side presence with teams in over 20 developing countries, and built partnerships with the “third estate” of all other market actors who affected the market without directly buying or selling—including opinion leaders and activists, regulators like the WHO and U.S. FDA, donors like PEPFAR and the Gates Foundation.
Consider as an illustrative example the challenge of stewarding the market through a major paradigm shift with the advent of next-generation ARVs. In the early years of HIV treatment scale-up, the fastest path to wider access was to put everyone on a stavudine-based drug regimen that was the cheapest on the market, yet very sub-optimal. The stavudine regimen had to be taken twice a day (reducing treatment adherence rates), could cause significant side effects, and produced less than ideal viral suppression. Better drugs were emerging, principally in the form of tenofovir-based regimens that offered better treatment outcomes but substantially higher pricing (initially ~5x higher). The Gates Foundation and many other opinion leaders argued against shifting patients to the newer regimens, saying they were intrinsically too expensive and would just mean fewer people accessing treatment.
A range of voices—including activists, PIH, MSF, and CHAI—came together to urge the global health community to play the long game. If we could accelerate demand for and roll-out of the tenofovir-based regimens, the price premium would eventually disappear.
Yet so much had to happen to pull off the shift to tenofovir regimens. CHAI’s presence on all sides of the market enabled it to quarterback the effort, coordinating across all the different actors involved and improving information flows. Within the same year CHAI helped parallel process many things that would otherwise have happened in serial:
Urging generic manufacturers to submit dossiers ASAP to the WHO and FDA
Influencing the WHO international HIV treatment guidelines process to recommend tenofovir-based regimens
Writing lengthy memos to Bill Gates to convince him that his skepticism on tenofovir-based regimens was unwarranted
Re-working demand forecasts with partner governments to plan the progressive shift in procurement
Aggregating that new demand and securing tens of millions in funding for the first wave of pooled tenofovir regimen procurement
Re-training health workers to prescribe the new regimens
Harmonizing regulatory requirements across developing countries to speed adoption
Under normal circumstances, these things would have eventually happened—but stepwise, one thing progressively leading to the next, and very slowly. The result of the concerted push was a much faster-than-expected market shift, from a three-pills-a-day regimen that sucked for patients to a one-pill, once-daily regimen with great outcomes. The 5X price premium fell to 3X quickly, and eventually fell even below the prices that had prevailed for the old stavudine regimens before the market shift began.
Phase 3: A maturing ARV market
Over the 10-15 years, the ARV market has continued to grow tremendously in lockstep with the roll-out of HIV treatment across the developing world. CHAI estimates a $2B developing-world ARV market size in 2020. Generic ARVs dominate supply and quality concerns have largely been put to bed.
CHAI and others have continued to engage in market-shaping to steer the market toward the healthiest dynamics and best patient outcomes. We’ve since gone through another evolution in the dominant first-line regimen–still including tenofovir but now with another powerful new drug called dolutegravir integrated into the triple-therapy cocktail—and seen prices for this regimen fall below $75 per patient annually. The community has tried some new tactics, including dose reduction and volume guarantees (a form of sales insurance that nearly eliminates demand risk for suppliers without the guarantor engaging in actual procurement). And ARV market-shaping successes have helped build appetite for market-shaping initiatives in other disease areas, including the pneumo vaccine AMC, the AMFm subsidy to accelerate uptake of artemisinin-based combination therapies for malaria, the Global Fund’s Pooled Procurement scheme, and many more. But for the most part, the global health community has been expanding upon the approaches proven out during the first couple of ARV market phases outlined above.
Parallels with carbon dioxide removal
Why should CDR folks take any interest in this short history of market creating and market shaping in global health? As different as they are, there are some lessons to draw out.
Collective imagination and thinking big
When we face the biggest challenges humanity ever has, we need to be making the most of our species’ unique superpowers of fictive language and collective imagination. In 2002, anyone saying we’ll have 30 million people on sub-$100 HIV treatment within 20 years would have been laughed out of the room. If you step outside the tiny world of CDR believers today and tell people we’ll have a trillion dollar CDR industry by midcentury removing 10+ gigatons of CO2 a year and consuming a third of the world’s total energy production, you might get the same reaction.
But it was the think-big, do-what’s-right, damn-the-torpedoes voices in the early years of HIV treatment who changed the conversation forever. Seemingly outrageous goals like 3 by 5 stretched the community’s sense of what might be vaguely-maybe achievable and the “Overton window” of policy conversation. Even those of us who allow ourselves to dream often need to push our own thinking—to make the next experiment even bolder, to set next year’s target even higher. Think XYZ is a crazy stretch? Think again.
Market shaping on top of market creation
Our challenge for the next thirty years isn’t merely to create a big CDR market, but to relentlessly shape it into the market we need. There are so many potential outcomes we could wind up with: a decent-size market but with major demand constraints; a huge market but largely concentrated in wealthy countries and with big pockets of questionable quality … at this infancy stage, lots of scenarios are believable.
So often, the outcomes and dynamics we end up seeing in free markets left to their own devices can be unhealthy or at least sub-optimal. We saw this movie in the ARV market and we’re seeing it again in the voluntary offsets market. Like a toddler, it’s amazing what a growing market can magically figure out on its own … and it shouldn’t be left unattended for too long.
At every step, we need to be active shapers of the market and not takers of market dynamics as they currently exist. And the more influence any given CDR market actor has, the more responsibility it bears for stewarding the market toward the vision we have for the future. Once the virtuous price/demand cycle really kicks in, the market will continue snowballing—but the snowball can roll in many different downhill directions.
Iterative technology paradigm shifts
Just like the evolution in dominant ARV regimens, from stavudine to tenofovir-version-A to tenofovir-version-B, the leading CDR technologies in 2025 are unlikely to be the winners in 2045 or 2065. And, critically, the general pattern will be for the next-generation technologies to enter at the high end of the price spectrum before coming down the cost curve with growing deployment. We generally won’t have the luxury of classically disruptive CDR technologies that attack from the “low end” of the market. So the chicken-and-egg problem will be a recursive one.
We can’t let ourselves become prisoners of what’s working today, as we almost did with very patient-unfriendly stavudine ARV regimens. We need to re-shape the market again and again, even when it feels like we’re swimming upstream or putting hard-won gains at risk. Even as some CDR companies start to hit sub-$100 prices at commercial scale, we need to be careful not to prematurely kill—or let languish—next-generation CDR possibilities in their infancy just because they are speculative, high cost, and have big MRV issues to sort out.
Cost!Cost!Cost! and Speed!Speed!Speed!
Just like PV panels and lithium-ion batteries—yet even more dramatically so—the coming decades of CDR (if successful) will need to be a sprint to ramp up deployment and translate that deployment into learning that helps wring every last ounce of cost out of the system. Plenty of companies or industries say or think they move fast, or that they’re relentlessly focused on cost reduction, but to actually push what Jigar Shah calls “deployment-led innovation” to the hilt is an incredibly demanding and rare discipline. This Shayle Kann podcast discussion with Raffi Garabedian (former CTO of First Solar) captures that discipline well.
I’ll never forget the moment a young colleague reported to our CEO Ira that, having done some diligence, he didn’t think our partner generic suppliers could ever beat Abbott’s low-income country pricing of $500 per patient per year for a drug called lopinavir/ritonavir. Ira paused for a beat, and said: “You don’t get it. You’re not thinking aggressively enough.” Two years and many tactics later, our partners announced a price just under Abbott’s; fifteen years later the $500 level is now a distant memory.
Quarterbacking
Maximizing the pace of the market’s evolution toward the promised land requires concerted and aligned action across many players in the market, and architecting this action such that steps happen in parallel rather than serial whenever possible.
What our experience in global health teaches us is that it’s easier to pull that off with a quarterback taking the lead on coordination. CHAI played that quarterback role in the ARV market, without being a huge buyer (except for time-limited periods to catalyze change in specific corners of the market) or a supplier or a regulator. CHAI established and used its soft power—flowing from its relationships and the track record it built—to change the behavior of market actors again and again by cajoling, informing, negotiating, supporting, and more. Others took on aspects of quarterbacking at times, though even in those instances CHAI coordinated closely with other ‘co-quarterbacks.’
In the CDR industry, which will ultimately become much larger and more heterogenous than the ARV market, it seems much less likely that a single leading quarterback will spearhead most of the market shaping. As I’ll discuss more in my next post, Frontier will—because of its heft—be thrust into the most prominent market steward role for the coming years. How and where things evolve from there is anyone’s guess. As a mega-buyer, Frontier’s positioning will be quite different than CHAI’s, yet it will have even more leverage to market-steer for the foreseeable future. Meanwhile, niche quarterbacks are starting to emerge in particular CDR technology zones—like the powerful and fascinating role Additional Ventures is starting to play in ocean alkalinity enhancement.
False binaries
Wired to simplify and impose stories on a messy reality, our minds easily seduce us into either/or framings that get in the way of progress. When there are multiple pathways, the dialogue becomes “stavudine versus tenofovir” or “prevention versus treatment.” In the early days of HIV treatment, those who passionately believed that we needed to prioritize prevention above all else felt it would be huge mistake to start down the treatment scale-up path. In their minds, scaling up treatment was both doomed to fail and so long as the fool’s errand was pursued would steal resources and leadership attention from prevention programs. Sound like anything you’ve heard in the climate space?
And again, even those of us who think we see the light aren’t immune. We may see with clear eyes and full hearts that the world needs to pursue CDR aggressively in parallel with reducing emissions; but we may still get lured into “nature-based versus engineered” or “maximize shots on goal versus double down on emerging winners” or other lines of reductionist thinking. I’ve met a lot of CDR folk who are drawn to the intellectual clarity and moral high ground of a ton of carbon unimpeachably and permanently removed from the atmosphere. Reality will be messier. Joining the CDR fray professionally is choosing to embrace paradox.